
| ACCUEIL |
|
Publié sur :
Gerard Rosen - 2001
Voir la version PDF de cette publication : Preoparative highdose chemptherapy for glioblastoma Charles Forsher, Todd Landman, Gerard Rosen Preoperative highdose chemotherapy for glioblastoma: report for 6 year disease-free survivalAbstractA 25 year old male presented with a residual 3x3cm growing mass 1 month after the incomplete resection of a large glioblastoma multiform (GBM).After he refused radiation therapy (RT) chemotherapy was started with high dose methotrexate ( HDMTX ) at the dose of 12 GM/M escalating to 30Gm/M with leucorvin rescue ( LR ) givent sequentially with hight dose carboplatinium ( HDC ) followed by autologous peripheral cell reinfusion ( PSCR ). After 6 courses of HDMTX with LR and 2 courses of HDC and PSCR one dose of stereotatic RT was given to the residual ( less that 1 cm ) mass. One month later, complete chirurgical resection of te lesional aera was performed. Because of wide resection through the ventricle, 2 doses of HDMTX ( 30 GM/M ) with LR were given post-operatively. Over six year later, the patient is alive with no evidence of recurrent disease. He never received other RT, and has normal cognitive and neurologic function. Based upon this experience, a trial of preoperative chemotherapy and fractionned stereotactic RT prior to ( and making possible ) a curative surgical procedure is proposed for the treatment of GBM. This model to curable through the use of effective prepoerative therapy is an extension of our successfull treatment of bone and soft tissue sarcomas. IntroductionHigh grade gliomas are cured only by total microscopic surgical removal but surgery is hardly ever curative because of residual infiltrating microscopic disease, or because of tumors that are too big to tataly remove without devastating neurologic sequelae. In the past 30 years the cure rate has not been incrased with all types of postoperative radiation therapy and chemotherapy. These modalities can only modestly increased survival, the quality of greatly diminished by effects of irradiation on normal brain tissue. Purpose of StudyTo utilize preoperative chemotherapy to reduce size of the tumor. This action occurs at the rapidly growing microscopic invasion of surrounding brainas the tumor shrinks. Preoperative sterotactic irradiation can further shrink the tumor and produce reactive gliosis around the residual mass, making delayed surgical removal potentially curative.  Large enhancing mass: Biospy showed "high grade glioma"  Residule/recurrent tumor 2 MO. After attempted removal at UCSF surgical speciment was read as glioblastoma mutliform. 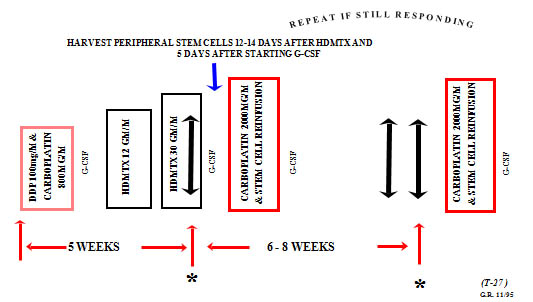 Preoperative chemotherapy was given for 6 Mo. Followed by single dose stereotactic RT 2Mo. Later surgery was performed. 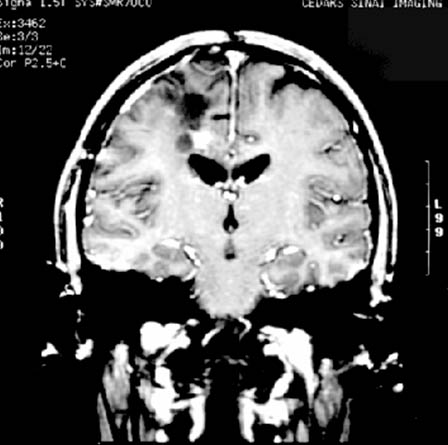 Response to preoperative therapy ( 8 Mo after recurrence ).  After curative resection chemotherapy was stopped after 2 more doses of HDMTx ( 30 Gm/m2 ) last neg. MRI march 2001. Treatment Strategy1-Biopsy ( stereotactic ) only to avoid wide field tumor contamination. 2-Agressive chemotherapy ( very high dose methotrexate and high dose carboplatinium with stem cells ). 3-Stereotactic RT ( Fractionned ). 4-Radio-enhancing chemotherapy ( HDMTX ). 5-Curative surgery. Advantage of this treatment strategy1-Potentially can increase the cure rate for high grade gliomas, at the very least increases quality ovarall survival. 2-Limited chemotherapy ( with low carcinogenic potential ). 3-Limited dysfunction and normal brain tissue necrosis. Conclusion1-This different approach is: -Feasible -Tolerable in all age groups -Potentially curative 2-With modern medical management "emergency surgery" is seldom necessary 3-Preoperative therapy has no detrimental effect on eventual surgical recovery. |
||
|
|
© Nicole Delépine - Biographie - Avocat famille Angers - Webangelis - Voyance |