
| ACCUEIL |
|
Publié sur :
Biomed & Pharmacother 44,217-224 - 1990
Voir la version PDF de cette publication : Results of multidisciplinary limb salvage in 240 consecutive bone sarcomas. G. Delépine, J.C. Desbois, G. Mathé, H. Cornille, Nicole Delepine Results of multidisciplinary limb salvage in 240 consecutive bone sarcomasSummary :From 1979 to 1989, 240 bone sarcomas of limbs were treated by a multidisciplinary limb salvage protocol. The tumors included 112 osteosarcomas, 71 chondrosarcomas, 3 fibrosarcomas, 10 malignant histiocytofibromas, 40 Ewing's sarcomas and 4 other rarer sarcomas. Patients mean age was 28.6 yr (range 4-91yr). The average tumor size was 13.5 cm (3-43 cm). There were 2 grade lA, 21 lB, 1 liA, 188 lm, and 28 III B according to Enneking's classification. Extratumoral en bloc resection was performed in ail cases (large in 113, marginal in 121, intrafocal in 6) by the same surgeon. In poor responders to preoperative chemotherapy with Ewing's sarcomas or osteosarcomas, 35 Grays postoperative radiotherapy was administered. Ewing's sarcomas and osteosarcomas received short preoperative and long postoperative chemotherapy. At last follow-up (median 60 months, range 6-120 months), 150 patients were disease-free; 4 were under treatment and had visible disease; 86 had died. Actuariat disease-free survival rate for patients seen with localized previously untreated disease was 83% at 2 yr and 77% at 3 yr. Fifteen local recurrences were observed (6%). Statistical analysis confirmed the poor prognosis factors of visible metastasis, proximal location and large tumor size, and pointed out the major prognostic value of therapeutic factors: the effectiveness of chemotherapy in Ewing's sarcoma and osteosarcomas, and the adequacy of surgery in ail cases. Limb salvage can be performed by a weil experienced multidisciplinary team in 96% of limb sarcomas without major risk of local recurrence. However, amputation is safer if the surgeon Jacks experience. Résumé :Résultats de la chirurgie conservatrice multidisciplinaire dans 240 cas de sarcomes osseux. De 1979 à 1989, 240 sarcomes osseux des membres ont été traités par les auteurs avec un protocole multidisciplinaire conservateur. Histologiquement, il s'agissait d'ostéosarcomes dans 112 cas, de chondrosarcomes dans 71 cas, de sarcomes d'Ewing dans 40 cas, d'histiocytofibromes malins dans JO cas, de fibrosarcomes dans 3 cas et de tumeurs diverses dans 4 cas. L'âge moyen des patients était de 28,6 ans (4-91). La taille moyenne des tumeurs selon leur grand axe était de 13,5 cm (3-43). Selon la calssijication d' Ennecking, il y avait 2 tumeurs de bas grade de malignité localisée à un compartiment, 21 tumeurs de bas grade de malignité extracompartimentales, 1 tumeur de haut grade de malignité localisée à un compartiment, 188 tumeurs de haut grade de malingité extracompartimentales, 28 tumeurs déjà métastatiques et extracompartimentales. La résection monobloc extratumorale a été réalisée dans tous les cas par le même chirurgien. L'examen histologique a montré que cette résection était large dans 113 cas, marginale dans 121 cas et contaminée dans 6 cas. Une radiothérapie post-opératoire à 35 grays a été utilisée chez les mauvais répondeurs à la chimiothérapie néo-adjuvante des sarcomes d'Ewing et des ostéosarcomes. Les sarcomes d'Ewing et les ostéosarcomes ont été en effet traités par une chimiothérapie pré-opératoire courte et une chimiothérapie postopératoire longue. Le recul moyen est de 60 mois (6 à 120). 150 malades sont vivants en rémission complète, 4 sont encore en traitement et 86 sont décédés dont 81 de leur cancer. La survie actuarielle des malades, vus avec une maladie non métastatique non précédemment traitée, est de 83% à 2 ans et 77% à 3 ans. Quinze récidives locales ont été observées (6%). L'analyse statistique confirme le mauvais pronostic des métastases visibles, des localisations proximales (bassin, fémur supérieur) et des grosses tumeurs. Surtout, cette analyse statistique souligne la valeur pronostique très dominante des facteurs thérapeutiques, l'efficacité de la chimiothérapie .dans les sarcomes d' Ewing et les ostéosarcomes, la qualité de la chirurgie (y compris la biopsie) dans tous les cas. Ce travail montre que la chirurgie conservatrice peut être réalisée pour 96% des sarcomes osseux des membres sans risque majeur de récidive locale, à condition de travailler en équipe multidisciplinaire expérimentée au recrutement mensuel suffisant. t:amputation est plus rare si l'équipe manque d'expérience. Introduction :Results of limb salvage surgery in sarcoma are often evaluated by multicentric studies where surgical procedures, adjuvant therapies and follow-up are insufficiently homogeneous to permit definitive conclusions. This study, based on 240 consecutive cases of limb sarcoma, treated by the same team, attempts to answer the main questions regarding limb salvage in bone sarcomas: how often is it feasible? Is-it worthwhile? Isn't it too dangerous? Patients and Methods :From 1980 to 1989, 240 bone sarcomas of limbs were treated by a multidisciplinary limb salavage protocol. The tumors included 112 osteosarcomas, 71 chondrosarcomas, 40 Ewing's sarcomas, 10 malignant histiocytofibromas, 3 fibrosarcomas and 4 other rarer sarcomas. The tumor locations were distal femur in 61 cases, hip bones in 42, proximal tibia in 32, upper femur in 27, proximal humerus in 25, scapula in 9, and other bones in 44 cases. The average age of patients was 28.6 yr (range 4-91yr). The average size of the tumor was 13.5cm (range 3-43 cm); according to the Musculoskeletal. Tumor Society criteria (MSTS), the tumor was classified as grade lA in 2, grade lB in 21, grade liA in 1, grade liB in 188, and grade IIIB in 28 cases. One hundred and forty-nine patients were seen before biopsy (132 with localized and 17 with primary metastatic disease), 60 were referred for surgery after biopsy and/or chemotherapy, 20 after local recurrence and 11 after local recurrence and metastases. Methods :Surgical guidelines Ail resections were performed by the same surgeon, and their margins assessed by the surgeon and pathologist according to the following definitions. Radical (= extracompartmental) excision involves the whole anatomie compartment (bone and soft tissues) where the tumor is located, and any compartment possibly contaminated by tumor cells, either initially or as a result of biopsy. Wide excision includes a safe margin of healthy tissue ali around the tumor extension and biopsy contamination; pseudocapsule or reactive tissue must not be seen. In marginal resection, the excision cuts close to the tumor. In at !east one place the pseudocapsule (or the reactive tissues) is seen but not entered. A contaminated resection is defmed by involuntary opening of the pseudo-capsule, even at a single point). The weakest point of excision defines the efficacy of the operation: if during an operation, in which a wide excision was intended, the tumor is opened at one single place or if histologie examination reveals that the margins are invaded by tumor cells the excision is contaminated. One hundred and thirteen resections were assessed as wide, 121 marginal, and 6 contaminated. Adjuvant treatment was adapted to the histology, location of the tumor and the age of patient. Radiotherapy Poor responders to neoadjuvant chemotherapy with Ewing's sarcomas and osteogenic sarcomas received 35 Grays to the tumor bed (between 2 postoperative cycles of chemotherapy). Chemotherapy High grade sarcomas (high grade osteosarcomas, Ewing's sarcomas, dedifferentiated chondrosarcomas) were treated by neoadjuvant and post-operative chemotherapy (sinee 1986, DD1 protocol for osteosarcoma and DD2 for Ewing's sarcoma. Reconstructive procedures After tumor removal, functional rehabilitation required multiple surgical procedures: 15 vascular salvage, 17 composite pedicle graft for skin coverage, 192 major bone reconstruction. Reconstruction of bone defects was achieved by massive prosthetic replacement, massive allograft or combinations or the two; there were 6 entire femur, 30 upper femur, 65 lower or diaphysal femur, 28 pelvic, 32 tibial, 27 humeral (2 of them entire humeral) reconstructions. Follow-up Local follow-up of the initial tumor site was assessed by clinical examination, standard X-rays, CT scan, quantitative bone scan, and sometimes MRI or computed angiography. Follow-up assessment was based upon bone scan, Jung CT scan, and more rarely plasma lipid bound sialic acid leve!(LASA). Average follow-up after biposy was 60 months (range 6-120 months). Results :Postoperative complications Prolonged surgical procedures (average 3.5 h; range 1-13 h), significant blood loss (average 3 1, range 1- 12 1) the older age of sorne patients, the side-effects of neoadjuhnt chemotherapy, probably explain in part the peroperative or early postoperative complications in 19 cases (8%) leading to the discontinuation of adjunctive therapy in 15 cases, poor function (14 cases), secondary amputation [9] or death [3]. The difficulties and the severity of complications clearly indicate the necessity of adequate experience and the treatment of a sufficient number of patients before undertaking limb preservative surgery for bone sarcomas. Oncologie results Of the 240 patients, 150 are alive and disease-free, 4 are still under treatment, 81 have died as a result of their cancer, 3 have died from iatrogenic side-effects, and 2 have died from other diseases. Actuarial disease-free survival of the entire group is 73% at 2 yr, 67% at 3 yr, and 62% at 5 yr. Local control Of the 240 patients, only 6% (15) suffered from local relapse. Most of the cases were complicated by inadequate biopsies which bad been performed in other centers, or limb salvage after local relapse in patients previously treated by radiation or surgery. Functional results The late functional result was evaluated in 231 patients according to MSTS grading and was estimated as excellent in 109 cases, very good in 68 (29%) good in 31 (12%), and poor in 23 (9%). Functional results were related to bone, nerve and muscle defects, depending on the location and on the side-effects of treatment. In our practice, complete excision of an entire muscular compartment was exceptional; the functional defect was usually compensated by hypertrophy of the remaining muscle. Tendon excisions were poorly tolerated, but were only necessary in the case of large metaphyseal resections, reconstructed by classical metal prostheses [3]. In order to improve functional results of limb salvage surgery, we developed use of allografts, combined in most cases with titanium prostheses. Cadaveric allograft material was acquired with no particular regard for sterility, and was preserved by mild freezing (- 40°C) and sterilized with external irradiation immediately prior to use. With bone graft material present, a period of restricted activity is advocated after surgery, to aid muscle reinsertion. In the upper limb, activity was restricted for 45 days; and in the lower limb, for 90 days. Functional improvement secondary to muscle attachment was particularly evident in the case of humerus, tibia and upper femur. All conserved limbs were pain-free except in6 cases. The functional state of patients was far better than that following amputation which would have been the treatment proposed in the past. Prognostic factors The worst prognosis remains correlated with: metastasis noted at the first consultation: of 28 patients with metastasis at our initial staging, only 13 are alive more than 2 yr after completion oftreatment; proximal location of the tumor: disease-free survival (DFS), of patients with tumor location at the hip scapula or proximal femur is 30% compared to 80% disease-free survival in patients with other locations. In patients treated by neoadjuvant chemotherapy, an initia11arge volume tumor is a predictive factor of a poor histologie response and of disease-free survival. In fact large volume tumor is also the essential poor prognosis indication, as early diagnosis and treatment appear to be the most important factors to obtain good local and general results. The influence of treatment on outcome is very interesting: in osteosarcoma, prognosis essentially depends on the efficacy of chemotherapy; DFS is 60% at 5 yr with postoperative chemotherapy, and is less than 35% with adriamycin (ADR). Cisplatin (CDDP) combination as preoperative chemotherapy is 80% with TlO (with respect to short preoperative chemotherapy). With adaptation of methotrexate (MTX) dose to age and individual pharmacokinetics, the actuarial disease-free survi:val reaches 100% at 42 months. In this study as in others [4, 8, 12, 13], conservative surgery gives comparable cure rates to amputation. In Ewing's sarcoma, systematic "en bloc resection" of primary bone tumor seems to improve prognosis. In our data, actuarial DFS is 90% at 40 months for patients treated by an .en bloc resection and DD2 protocol. Compared to the previous pilot study (DFS 35% at 3 yr in patients treated by radiation and chemotherapy), these preliminary results are promising (fig 5). 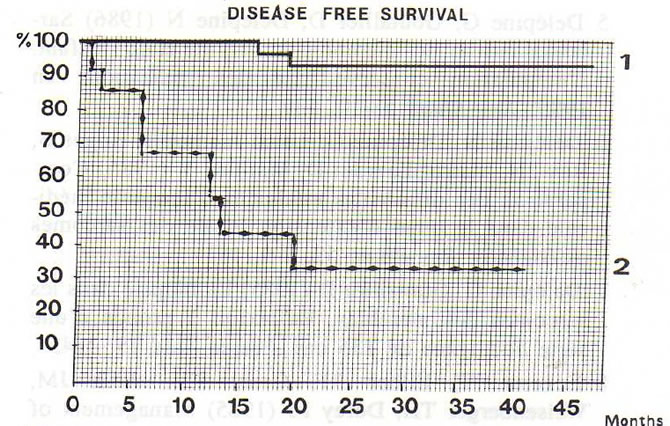 Fig 5. Actuarial disease-free survival of Ewing's sarcoma ac cording to 1), radiotherapy and chemotherapy protocol; 2), protocol DD2 with en bloc resection. In low grade (I or Il) chondrosarcoma, the major prognostic factor appears to be the early surgical treatment and the quality of surgical en bloc resection [2, 9, 11, 14]: if local control is obtained by the first treatment DFS is 90% at 5 yr, but only 60% after local recurrence (fig 6). Regarding surgical margins, in this study radiotherapy was generally used for poor responders; the local recurrence rate was not greater for marginal resection (121 patients, 6 local relapses) than for wide resection (113 patients, 5 local relapses). The most important surgical factor in avoiding local relapse is the extratumoral quality of en bloc resection outside the limits of the tumor. It is essential not to open the tumor (4 local relapses occurred among the 6 contaminated resections). 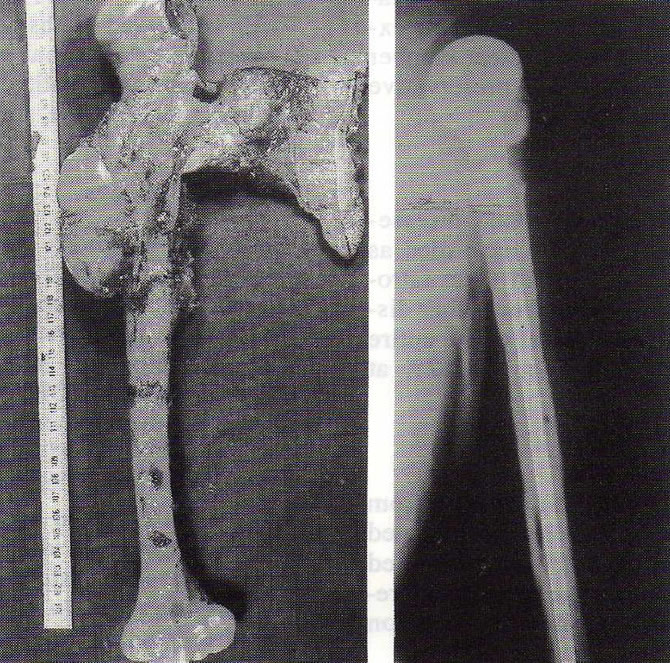 Fig 1. Total humeral replacement for fibrosarcoma. Functional result rated excellent. There has been complete remission for 4 years. 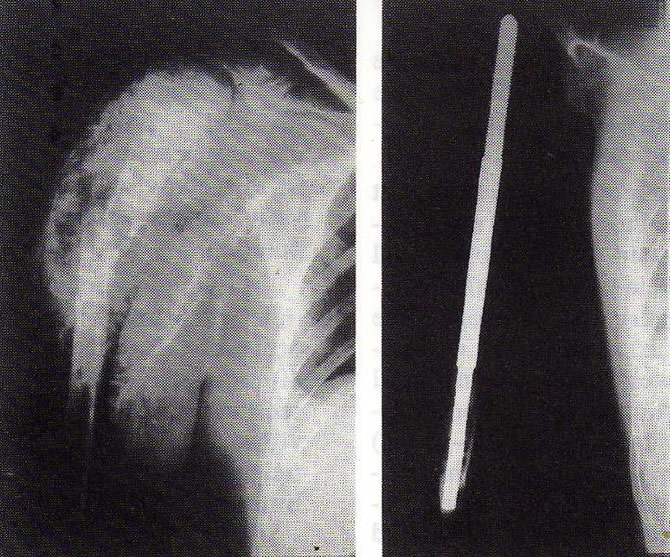 Fig 2. Pathologie fracture of a humeral osteosarcoma. En bloc resection and prosthetic. replacement. Good result 98 months after resection. 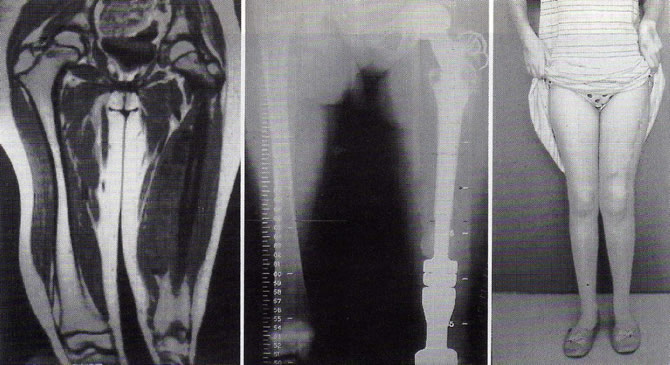 Fig 3. Large Ewing's sarcoma of the femur. En bloc resection of the total femur, growing prosthesis coated with bank allograft. Good functional result after 2 years. Discussion :Which are the most important questions concerning limb sparing surgery in limb sarcomas? Isn't it too dangerous? Is the functional result worthwhile? Is it feasible ? Risks of conservative surgery Risk of recurrence is naturally included in conservative surgery. In fact, only 2 factors are essential in making a decision as to whether the limb should be spared or not. The surgeon's experience and the efficacy of the adjuvant treatment. The sensitivity of permeation nodules to adjuvant treatment depends on the type of tumor: local relapses are more frequent in high grade fibrosarcomas and chondrosarcomas than in osteosarcomas and Ewing's sarcomas (when seen before biopsy). Initial treatment procedures are the most important factor determining local prognosis: in our study, local relapses occurred in 4% of cases (6!149) in patients seen before biopsy, but in 10% (9/91) in patients seen after biopsy [7]. Tumor size, pathological fracture, and young age were not correlated with risk of local recurrence. Functional advantages The functional advantages recommend the use of conservative surgery. Ninety-five % of our patients are living far better than they could have done after amputation. This functional advantage increased inversely with the tumor size as surgery is, in our practice, as "conservative" as possible, guided by sophisticated computed imaging [6] and protected by routine adjliVant local radiotherapy in poor respondeu. Social and professional problems, affective persona! relationships are also greatly improved. 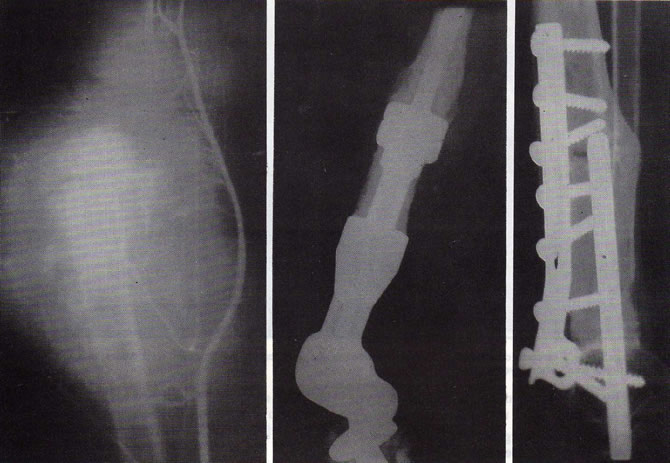 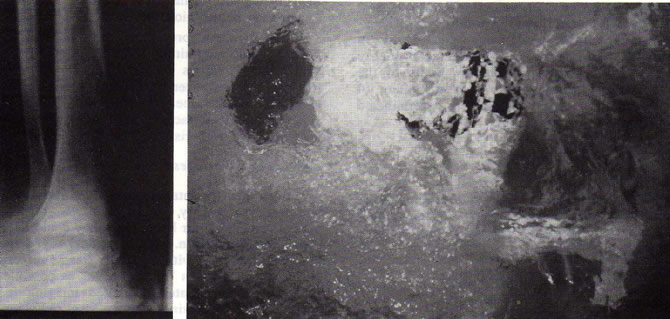 Fig 4. Multifocal osteosarcoma. En bloc resection of the 3 visible bone metastases. Functional result rated as excellent 5 years after operation. 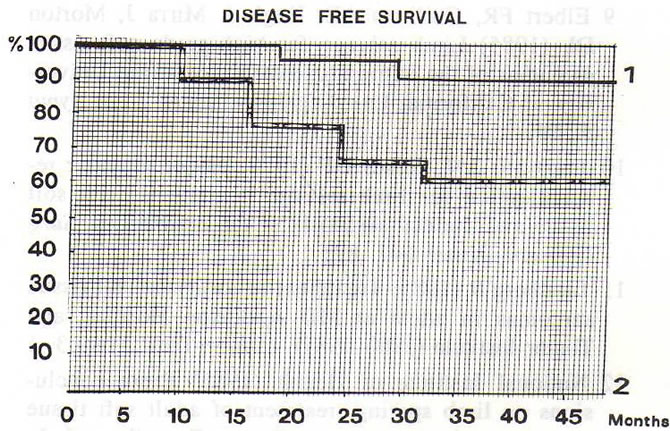 Fig 6. Actuarial disease-free survival of low grade chondrosarcoma accordinto initial treatment. 1), patients initially treated by our team; 2), patients referred afer local recurrence. by conservative surgery. Psychological support cannot replace the amputated limb; and it is not over enthusiastic to state that conservative surgery preserves quality of life in young children or teenagers during a particularly difficult period of their lives. Amputation, although fast is often followed by divorce, or being turned away by friends, chronic rejection and indifference towards rehabilitation and possibly loss of job. Another major advantage of conservative surgery consists of the improvement in contact between doctor and patient. Limb sparing leaves the patient in a physical and e otional state that makes them receptive to adjuvant chemotherapy as long as is necessary and which largely compensates for the local recurrence risk of the method. Is conservative surgery often feasible? "Feasibility" essentially depends on the surgeon's determination, experience and ingenuity. The surgeon and his staff must assess each case without an a priori. Each operation should be adapted to the age of the patient, to tumor size and location and to probable vascular and skin complications [5]. To emphasize these fondamental principles, we will analyze the classical contraindications regarding conservative surgery. Young age of the patients is no longer a contraindication as procedure planning will program limb equalization during growth. Our patients with osteosarcomas or Ewing's sarcomas have benefitted from an expandable prosthesis which permits compensation of discrepancy of length of the limb. Tumor size > 15 cm length requires longer procedures, lowers the final functional limb value and overall prognosis, but does not increase local recurrence rate. As the functional result remains far better than amputation, limb sparing procedures are still justified (fig 1, 2, 3). Failure of neoadjuvant chemotherapy leads to a high risk of metastasis but does not increase the local recurrence risk, providing that local radiotherapy follows surgery. Pathological fracture does not increase the recurrence rate if conservative surgery is performed 2 or 3 weeks after orthopedie treatment, and if the en bloc resection does not open the fracture hematoma and removes it together with tumor (fig 2). Multifocal locations of osteosarcomas or metastatic osteosarcoma are not good indications for amputation, if en bloc resections of all visible locations are feasible (fig 4). Vascular involvement requires vascular reconstruction by vascular repair performed in various ways with the help of a vascular surgeon for this part of the reconstruction process [10]. Infection following biopsy or conservative surgery greatly worsens the prognosis because it prevents chemotherapy from being administered and bone reconstruction from being carried out. If a femoro-tibial nailing with gentalline cement does not produce rapid improvement, amputation may be indicated. These infectious complications led us to carry out amputatioQs in 2 patients over a 10-yr period for concomitant vascular and skin involvement. Local relapse after radiotherapy greatly increases the recurrence rate following marginal exctswn. In this situation, conservative surgery could be performed only for very small tumors which permit wide en bloc resection. In our practice, amputation bas been discarded as routine treatment, and it bas been performed in only 12 patients over a 10-yr period (4% of cases treated during this period). Conclusion :Our pratice shows that limb sparing surgery can be performed in 96% of cases of bone sarcomas without major danger to life or local control, providing one is helped by sophisticated computed imaging and adjunct therapies, and that the team bas sufficient experience. In other situations (the non availability of medical imaging, no experience of such tumors, contraindications regarding adjuvant chemotherapy, recurrence in an irradiated field or infected wounds), amputation remains the wise solution. References :1 Campanacci M (1980) Local recurrence after amputation for osteosarcoma. J Bone J Surg 62 B, 201 2 Collin C, Godbold J, Hadju S, Brennan M (1987) Localized extremity soft tissue sarcoma: an analysis of factors affecting survival. J Clin Oncol 5, 601 3 Delépine G, Delépine N (1987) Titanium massive prosthesis combined with bone grafts. In: Bone Tumor Management (Coombs R, Fried Laender G, eds) Butterworths and Co Ltd, 28, 211 4 Delépine G, Goutallier D (1985) La resection dans le traitement des ostéosarcomes des membres. L'amputation conserve-t-elle des indications? Rev Chir Orthop (Paris) 71, 451 5 Delépine G, Goutallier D, Delepine N (1986) Sarcomes osseux des membres de l'adulte et de l'enfant. L'amputation conserve-t-elle des indications en 1985? Rev Rhum 53/10, 539 6 Delépine N, Delépine G, Laval-Jeantet B, Roger B, Buy JN, Vadrot Lazrdet D, Mathieu Y (1985) Comparaison des différentes méthodes d'imagerie médicale dans le bilan d'extension locale des sarcomes ostéogènes. Rev Rhum 52, 7-9, 463 7 Delépine G, Goutallier D (1985) La biopsie dans les sarcomes des membres. Réflexion à propos d'une série homogène de 135 cas. Presse Méd 15, 1145 8 Eckardt JJ, Eilber RF, Grant TT, Mirra JM, Weisenberger TH, Dorey FJ (1985) Management of stage liB osteogenic sarcoma: experience at the University of California, Los Angeles. Cancer Treat Symp 3, 117 9 Elbert FR, Guiliano AE, Hugh J, Mirra J, Morton DL (1985) Limb salvage for high-grade soft tissue sarcomas of the extremity: experience at the University of California, Los Angeles. Cancer Treat Symp 3, 49 10 Imparato AM, Roses DF (1978) Major vascular reconstruction for limb salvage in patients with soft tissue and skeletal sarcomas of the extremities. Surg Gynecol Obstet 147, 891 11 Lindberg R (1985) Treatment of localized soft tissue sarcomas in aduts at MD Anderson Hospital and Tumor Institute (196 1981). Cancer Treat Symp 3, 1 12 National Institute of Health (1985) Panel conclusions on limb sparing treatment of adult soft tissue sarcomas and osteosarcoma. Cancer Treat Symp 3, 1 13 Potter DA, Kinsella T, Glatstein E, Wesley R, White DE, Seipp CA, Chang AE, Lack EE, Costa J, Rosenberg SA (1986) High grade soft tissue sarcomas of the extremities. Cancer 58, 190 14 Simon MA, Aschliman MA, Thomas N, Mankin HJ (1986) Limb salvage treatment versus amputation for osteosarcoma of the distal end of the femur. J Bone J Surg 68-A |
||
|
|
© Nicole Delépine - Biographie - Avocat famille Angers - Webangelis - Voyance |