
| ACCUEIL |
|
Publié sur :
Congrès UICC, Olso - 2002
Voir la version PDF de cette publication : Long-term results of comprehensive treatment for non-metastatic primary limb high-grade osteosarcoma. Emphasis of escalating high dose methotrexate (HDMTX). G. Delepine, H. Cornille, B. Brun, S.Alkallaf, B. Markowska, Nicole Delepine Long-term results of comprehensive treatment for non-metastatic primary limb high-grade osteosarcoma. Emphasis of escalating high dose methotrexate (HDMTX).Purpose of this studyEvaluation of effects of escalating induction HDMTX on toxicity, response of tumours and survival of patients with osteosarcoma. 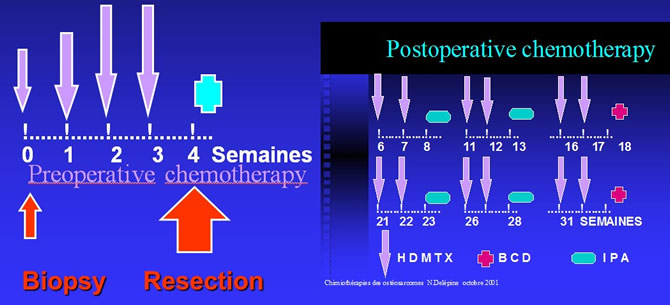 PatientsFrom 1/85 to 12/2000 : 46 patients with non metastatic limb osteosarcoma, previously untreated. 29 M, 17 F (7 - 30 y, mean : 16.6) were treated in one of AP-HP oncologic service. 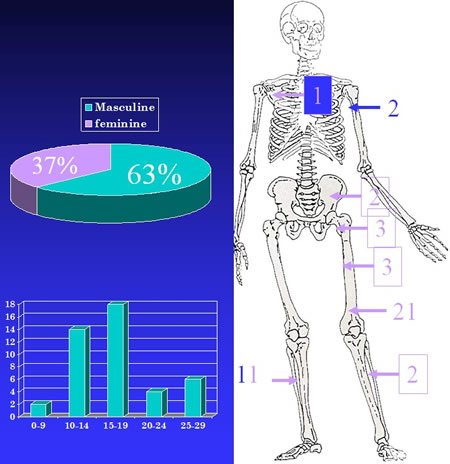 Size of the tumours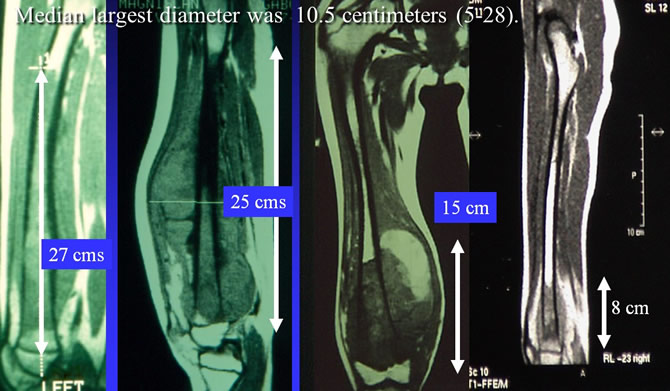 MTX dose of first courseMTX dose of first course was adapted to age : - 5-9 y : 18 g/m², - 10/15 y : 15 g/m², - > 15 : 12 g/sqm. For the same dose inter patient variability of serum peaks was high. 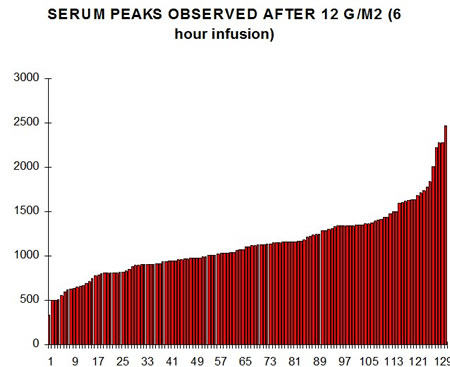 Dose escalation scheduleMTX was escalated from 2 to 4 gr/sqm if the serum peak H6 < 1000 µmol/l or in case of clinical ineffectiveness. 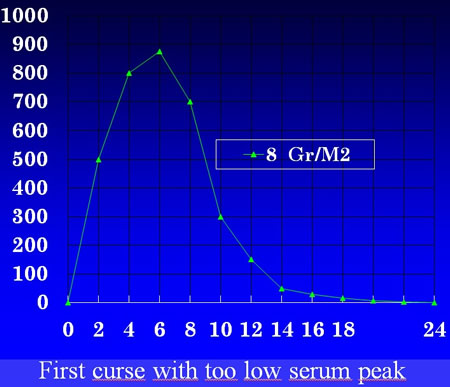 Correlation between H6 and doseIn each patient Correlation between H6 (µmol/l) and dose (gr/sqm) was linear. 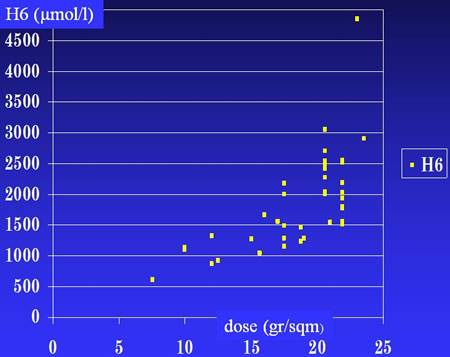 Frequency of dose escalationEscalation was necessary in 80 % of patients (37/46) due to low H6 (13), lack of clinical response (9) or both (15). 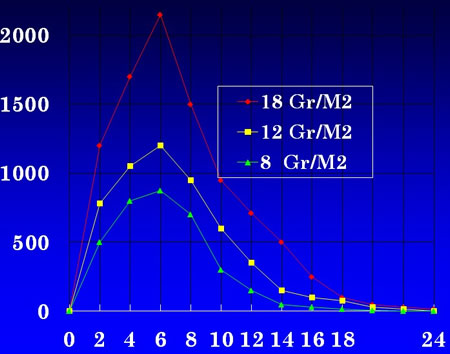 Preoperative dose escalationAverage increase of dose was 40 % p. received a mean preoperative dose : 14.3 gr/m²/course (8-24 g/m²), mean H6 : 1248 µmol/l (570-3600). Observed toxicityInduction therapy was well tolerated. The most frequent postoperative toxicity was hematologic grade 4 : 90 % of IPA (IFO, CDDP, ADR). Limiting factor of dose escalationHepatic toxicity was the main limiting factor of postoperative MTX. Observed in 60 courses of MTX (7 %) it resulted in early stopping of MTX in 4 patients. Radiological responses Good in 30 Stable disease : l2 Inevaluable : 4 Local treatmentAll patients were primarly treated by limb salvage even in case of : Huge tumor Young child Fracture. 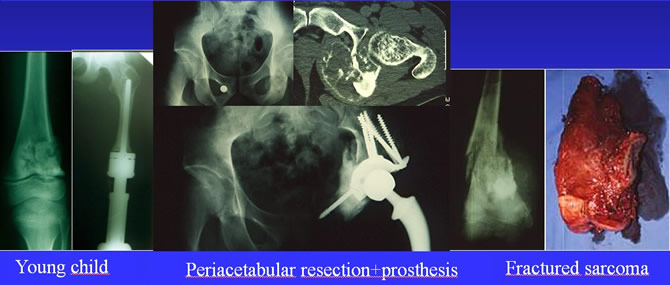 Histological ResponseGraded according Huvos and Rosen criteria was : good : in 25, bad : 21. Total doses of MTX therapyTotal doses of MTX therapy given dose of MTX Averaged 250 g/sqm in 41 wks. Mean MTX intensity 6.3 g/m²/week, Mean value H6 : 1380 µmol/l. Oncologic resultsRelapses : out of 46 patients, we observed one local and 7 distant relapses, 4 lung, 3 bone. Average time to relapse was 25 m. (8-75). Final outcome : 2 p. died, 2 p. are living with evolutive disease 42 others are in CR. 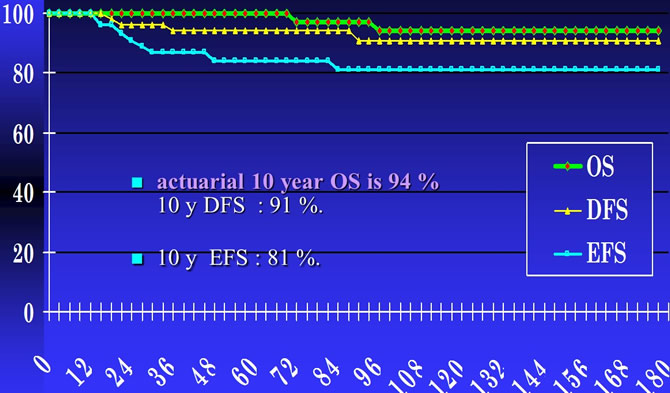 ConclusionsIn our patients escalating doses following Rosen's rules and pharmacokinetics monitoring permits : 1. The given dose of methotrexate, the dose intensity and the serum concentration X time, to be increased by 40 % in patients who needed it. 2. To increase the event free, the disease free and the overall survival rate of patients. 3. Without severe increase of toxicity. Protocols for OS should require not only a good total (> 240 g/sqm) dose MTX but a serum peak over 1000 µmol/l at after 6 hours infusion or 1450 µmol/l after 4 hours infusion. |
||
|
|
© Nicole Delépine - Biographie - Avocat famille Angers - Webangelis - Voyance |