
| ACCUEIL |
|
Publié sur :
XII national congress of tchek orthopaedics - Praha - 2008
Voir la version PDF de cette publication : Strategy of treatment of osteosarcoma. G. Delepine, Nicole Delepine Strategy of treatment of osteosarcoma.Surgery alone can cure only 15-20% of patients with localized high grade osteosarcoma. 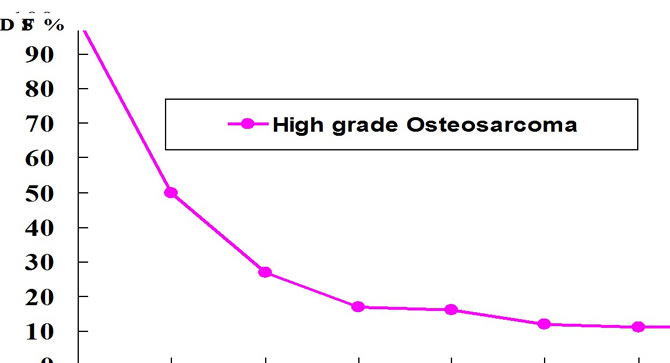 Sarcomata of the osteogenic Series Mac Kenna et coll...J.B.J.S. 1966,48-A ,1;1-26 Chemotherapy alone can never cure an osteosarcoma. N. Jaffe tried intensive, prolonged chemotherapy in patients with spine inoperable OS. After some stabilization all tumor recurred . Comprehensive treatment remains the gold standard but the optimal schedule of chemotherapy and surgery remains controversial. The aim of this review is to propose an optimal schedule of treatment based on Rosen's rationale and our own experience. Jaffe demonstrated the correlation dose intensity of Methotrexate/Response of OS. High Dose Methotrexate (HDMTX) administered every 3 weeks obtain 30% response. But 87% when administered every week at higher dosage. 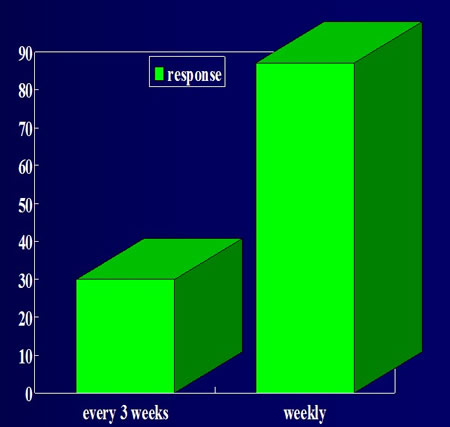 Récent advances in the chemotherapy of metastatic osteosarcoma, Cancer 1972,30: 1627. Weekly HDMTX and citrovum factor in osteogenic sarcoma, Cancer 1977, 39 : 45. Strategy of Rosen T5 protocol Rosen thought that the follow up of the tumor during chemotherapy could permit to realize an antimitogramme in vivo. He gave preoperative chemotherapy to determine the optimal dose for a particular patient.  Rosen G. and all. Primary Ostogenic Sarcoma .The rationale for preoperative Chemotherapy and Deayed Surgery. Cancer 43:2163-2177,1979. Preoperative chemotherapy permits to find "the optimal dosage" for individual patient. 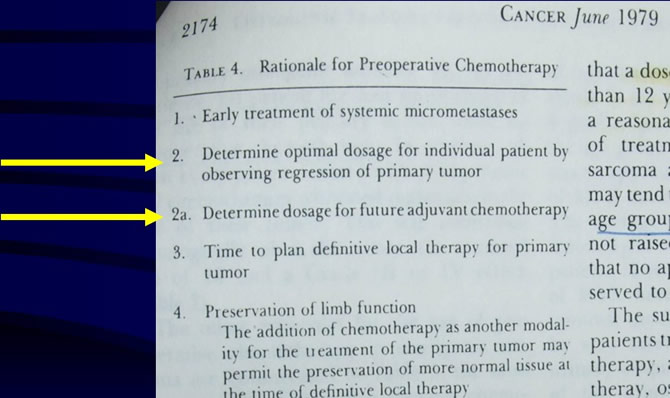 30 years ago G Rosen underlined that preoperative chemotherapy is an investigative method. Not a recipe. Allowed us to determine the optimal dose of HDMTX for each patient.  T5 protocol strategy was successful The T5 protocol based on pre and post operative HDMTX (8 G/m²) and Doxorubicin obtained 75% disease free survival. And permit to observe that children needed usually more MTX (12 G/m² vs 8 G/m²). 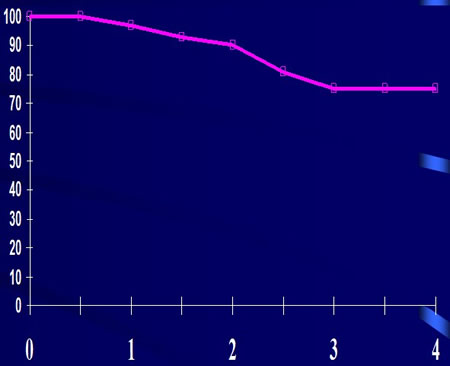 Rosen G. and all. Primary Ostogenic Sarcoma. The rationale for preoperative Chemotherapy and Deayed Surgery. Cancer 43:2163-2177,1979. Strategy of T7 In the T7 the first dose of MTX of children under 12 years was increased, while adults received 8 g/m². Postoperative chemotherapy was identique for good and bad responders defined on histologic examination of the primary resected after preop chemotherapy. Bad responders had a lower EFS than good responders confirming the rosen 's hypothesis that primary was representative of micrometastases. Strategy of T10 In the T10 protocol the postoperative chemotherapy was different for good and bad responders. Postoperative chemotherapy for good responders used the same drugs (HDMTX, Doxo,BCD) up to 20 curses of MTX. Bad responders continued on HDMTX but received a chemotherapy reinforced by CDDP instead of BCD. This post operative chemotherapy rescued the bad responders. T10 protocols were successfull 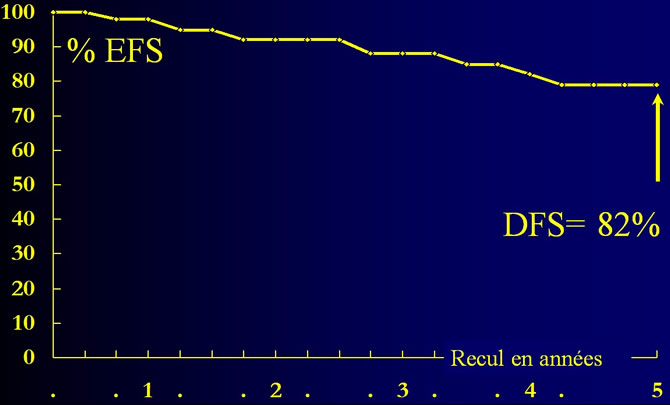 Rosen G., marcove R.C., Capparos B., and coll. (1979). Primary osteogenic sarcoma. The rationale for preoperative chemotherapy and delayed surgery. Cancer, 43, 2163-2177. But after he published his resultsthe medical community retains the recipe and forgot the underlying philosophy. In all multicentric trials a fixed dose of MTX was administered. And published results were all under Rosen T7 and T10. Results of SFOP "T10" 1979-1986 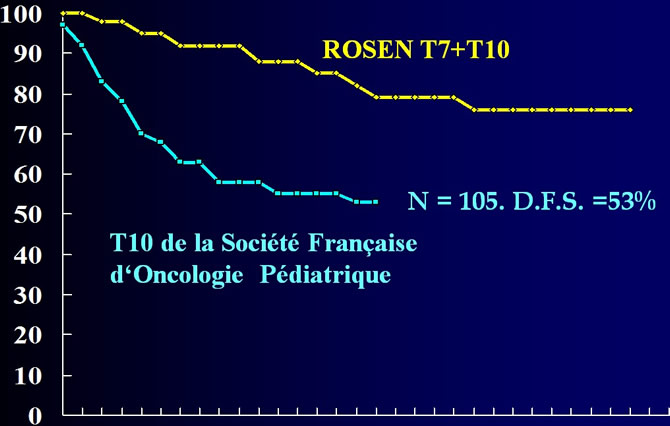 M.BRUNAT-MENTIGNY 1988 "La reproduction du protocole de ROSEN pour les osteosarcomes. Bull.Cancer 1988,75:201-206. EFS of patients in EORTC-EIO trials (vs Rosen) Mean value of EFS of 610 patients include in E IO trials is 46%. 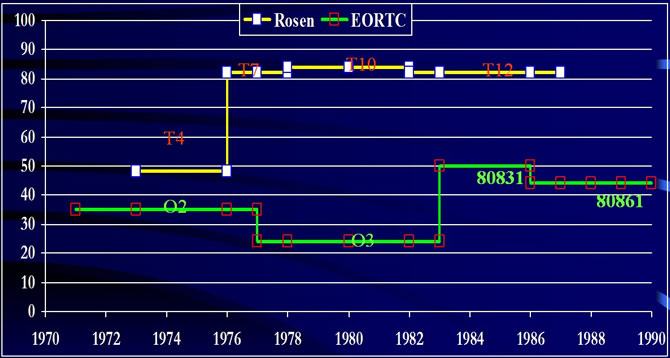 EFS of patients in american trials (vs Rosen) 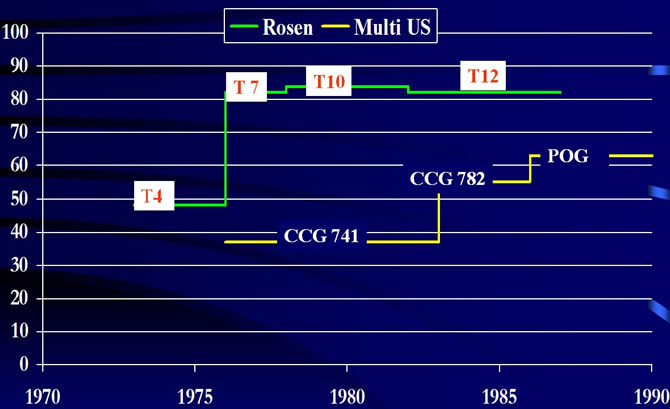 For more than 25 years a lot of multicentric trials on treatment of OS have been made Global results are disappointing both on scirntific and medical points of view : Very few hypotheses have been definitivly confirmed and very new concepts elmerged. Efs of patients did not increased significantly. Very few scientific data have been definitivly confirmed Discordant data have been published and do not confirm the major hypotheses of Rosen: Does Preoperative chemotherapy improve DFS? Is response predictive of DFS? Does HDMTX improve DFS? Which the optimal dose of HDMTX? Can postop chemotherapy rescue bad responders? Despite the quality of collegues, statisticians and methods, multicentric trials globaly failed Multicentric trials study the "mean patient" with the "meam osteosarcoma" supposing that all patients and all osteosarcoma are comparable. They ignore our metabolic differences. But we are all unique, all different. And osteosarcoma are all unique all different. Every human being is unique at birth. We are all different : 3 main races And so many others. When we grow our experiences (food, illness, medications, environmental status) are unique and increase our differences. We are all different, all unique: Different weights. We are all different, all unique: Different sizes. These differences are not well balanced by de dosage in gr/sqm We are all unique, all different. And also our pharmacokinetiks of anticancer drugs. 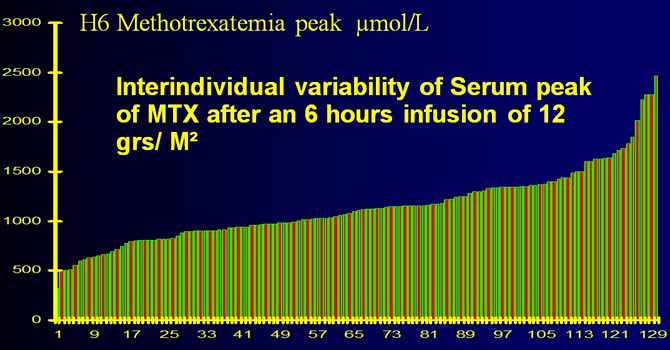 Pharmacockinetics of HD MTX. Conclusion about 622 courses performed in 4 years in children, teenager and adults. Nicole Delepine, G. Delepine, J.C. Desbois, H. Cornille, B. Brun, V. Subovici, S. Alkallaf, S. Nejmeh, C. Jasmin Medical and Pediatric Oncology Vol 17 number 4 - page 304 ; 1989. Tailoring the dose according individual PK permits to overcome the inter individual variability for optimal therapeutic use. If you infuse 12gr/sqm of MTX in 6 hours the peak of methotrexatemia can reach 2500 µmol /L or 350µmol/L resulting in increased risk of toxicity for some patients or ineffectiveness of treatment for others. But Osteosarcoma are all different, all unique. Many histologic subtypes : - commun type - anaplasic - chondroblastic - telangectasic - fibroblastic... Many radiologic subtypes. Many differents of cellular drug resistance. The presumed intrinsic MTX resistance has been ascribed to an impaired MTX polyglutamylation associated. In addition, MTX uptake may be defective as observed whereas also high levels of (altered) DHFR have been reported. Many differents of oncogenes expression. such situation is comparable to treatment of severe bacteriema Bacteriologists use pharmacokinetiks to adapt dose of antibiotics and antibiogram to evaluate the efficient serum concentration. Which drug ? Only two agents effective against osteosarcoma have a large therapeutic index permitting significant increase of dose : MTX and Ifosfamide. These two drugs demonstrated a dose/effect correlation on osteosarcoma. Why do we prefer HDMTX ? Methotrexate offers many advantages : It represents the only drug whose total dose and dose intensity are statistically correlated with 5 year disease free survival of patients it can be infused with a weekly interval, the pharmacokinetiks can be easily studied, the toxicity can be rescued by folinic acid, and aplasia is usually not a problem when Methotrexate is administrated in monotherapy. For these reasons we use only Methotrexate in preop CHT. We have observed that mean methotrexatemia during preoperative phase is correlated with response. 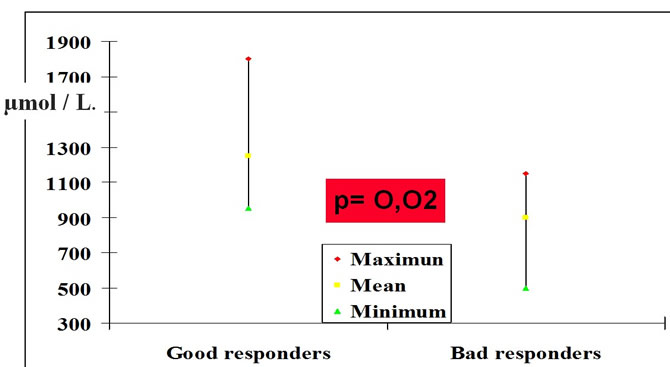 Correlation between seric methotrexate level and histologic response in osteogenic sarcoma. Nicole Delepine, G. Delepine, JC Desbois - Medical and paediatric oncology - Vol. 19 n° 5/1991 Scandinavian confirmed the correlation of methotrexatemia and histologic response 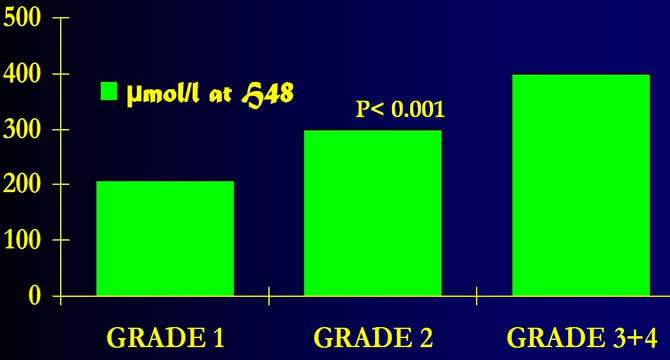 SOLHEIM O . "THE TREATMENT OF OSTEOSARCOMA :PRESENT TRENDS. Annals of Oncology 3 (suppl.2) S 7 -S 11. Scandinavian T10. Pronostic value of H48 methotrexatemia in grade 2 responders. 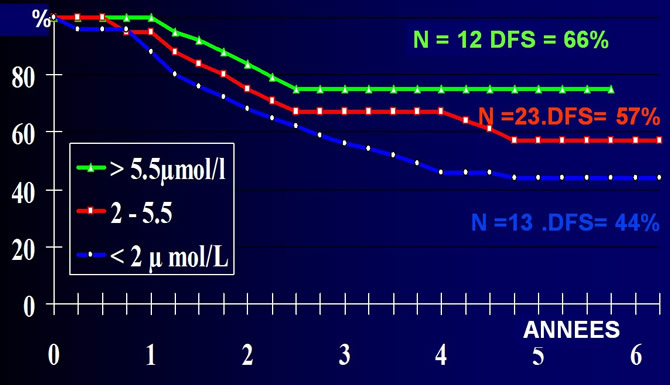 Saeter G. and all. "TREATMENT OF OSTEOSARCOMA. J.Clin.Oncol 9,10,1991:1766-1775. Pronostic value of H6 Methotrexatemia. PROTOCOLE RIZZOLI 2 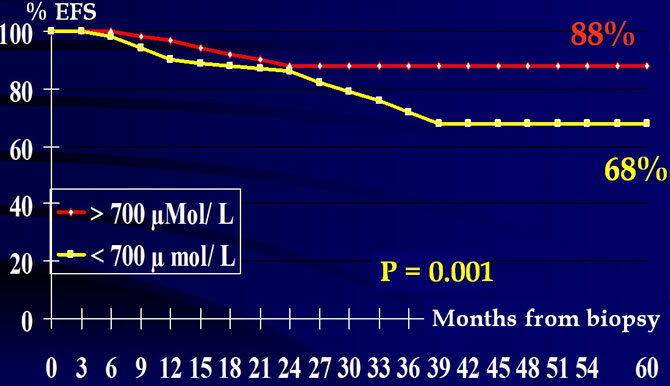 Bacci g.,Picci P., Ruggieri P. et coll. "Primary chemotherapy and delayed surgery for osteosarcoma of the extremities." Cancer 65, 2539-2553, 1990. GRAF N. Pronostic value of H4 methotrexatemia 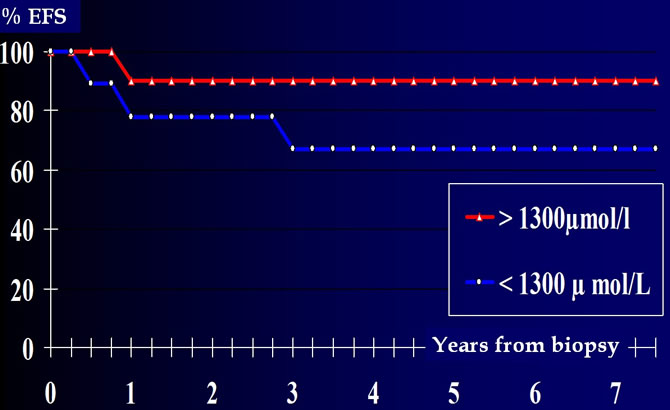 Graf N. and all.Einfluss der Methotrexatpharmakokinetik und Klin. Padiatr. 202 ; 1990:340-346. With Methotrexate, more you give, more you obtain. Correlation DFS/ Dose intensity of MTX 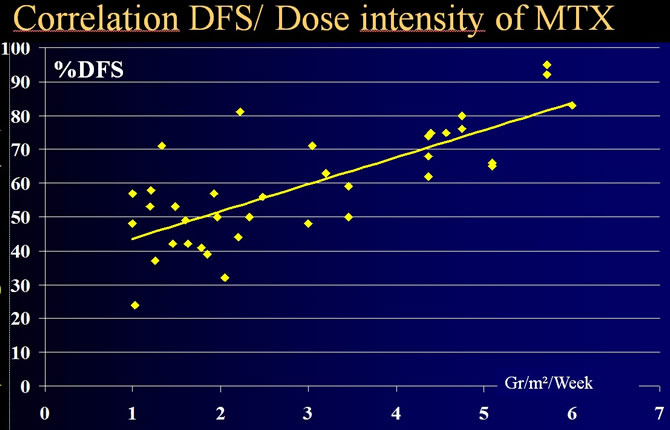 Delepine, Rosen, Bacci and coll Influence of methotrexate dose intensity on outcome of patients with high grade osteogenic osteosarcoma. A litterature analysis, about 1909 cases. Cancer, 1996, 78 : 2127-35. But no gold standard for dose of methotrexate Pharmacokinekics of patients are individual. Resulting for a fixed dose, in increased risk of toxicity for some patients and ineffectiveness of treatment for many others.  We tried to apply Rosen's rationale As soon after biopsy we start with HDMTX (8 to 15 G/Sqm according to age) with complete PK study. On D7 the second curse is administered with a tailored dose to obtain : A clinical response of the primary (decreasing of local hyperthermia and vascularisation). And a serum peak of 1000µmole/L. 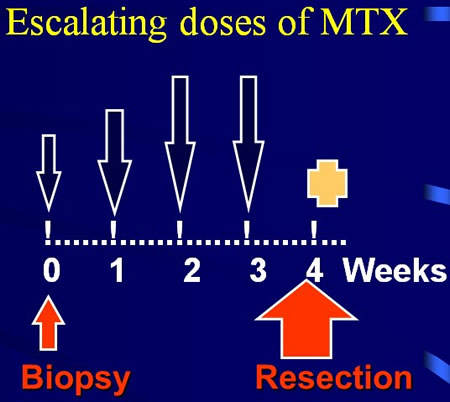 During preoperative chemotherapy the surgeon must evaluate the tumor every week We increase the dose. If the serum peak is too low. Less than 1000µmol/l if infusion of 6 hours. Rosen propose 1450µmol/l for an infusion of 4 hours. if pain or local hyperthermia remains. OS. DD protocols. Preoperative chemotherapy MTX doses are increased if the serum peak is too low of if tumor does not respond enough. 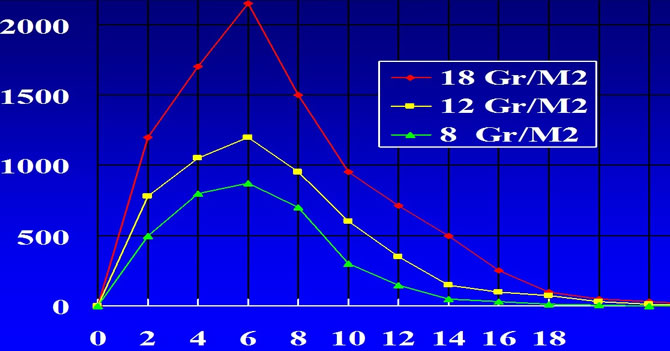 60% of our patients received escalating doses The mean increase of dose is 40%; We had sometimes to increase the dose up to 22 G/Sqm per curse. With such a method we always obtain clinical response of primary OS and never more observe progression of disease during preop chemotherapy. With a reinforced rescue they do not suffer of increased toxicity. Response of OS after short preop HDMTX 4 to 5 weeks of individualized curses of HDMTX are enough even in case of fracture. 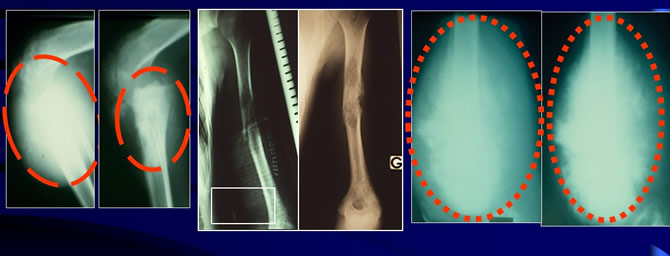 Lenght of preoperative chemotherapy? I seems safer to resect the primary as soon as the optimal dose of MTX has been evaluated by the preoperative chemotherapy. With MTX four to five curses in 4 to 5 weeks are enough. For that reason we always operate early after 4 to 5 weeks of MTX. Preoperative chemotherapy can be dangerous Too long preoperative chemotherapy may be dangerous if chemotherapy is not effective enough and may increase the risk of induction of chemoresistance and of metastases. All these patients died 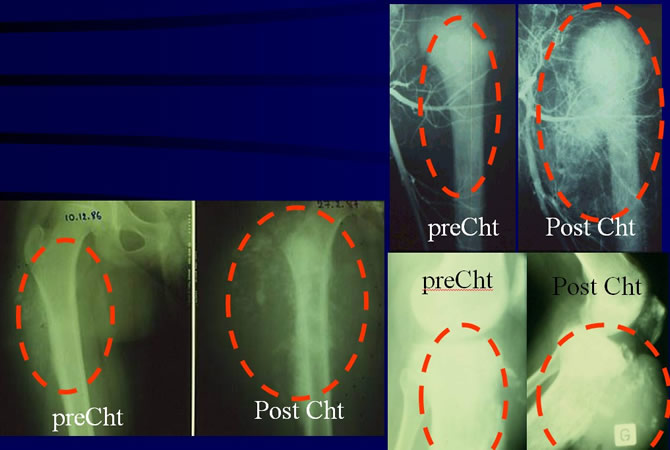 Postoperative chemotherapy Uses HDMTX (12 additional curses at the effective dose), IFO (3 curses with 12 G/Sqm), Tep Rubicin and CDDP (3 curse). We use the same drugs in good and bad responders. Bad responders received only one curse more. OS DD PROTOCOL. POST-OPERATIVE CHIMIOTHERAPY 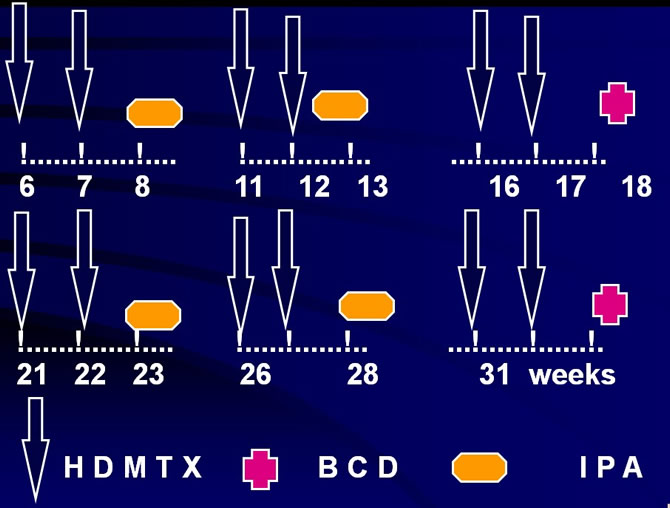 Our Résults 1982-2007 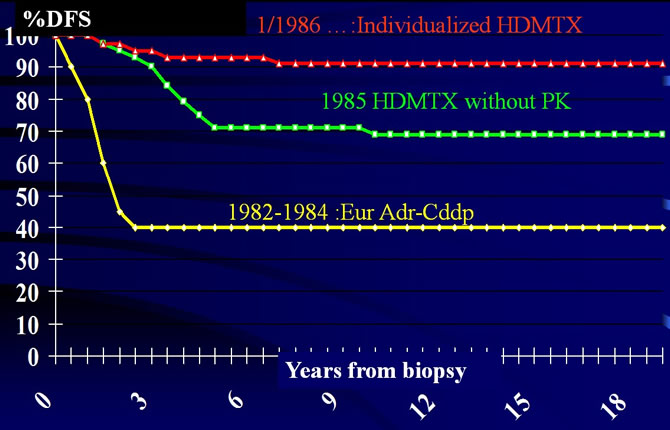 Conclusions We are all unique, all different. Osteosarcoma are all unique, all different. We all kwon that taylored suit fit us better than standardized suit. We treat severe infection with individualized antibiotherapy accorded to pharmacokinetiks and antibiogram. We should treat patients with individualised doses of HDMTX defined during the preoperative chemotherapy by examining the response of the primary. |
||
|
|
© Nicole Delépine - Biographie - Avocat famille Angers - Webangelis - Voyance |