
| ACCUEIL |
|
Publié sur :
Jorge. A Lazareff - 1994
Voir la version PDF de cette publication : H-MRSI and pediatric low grade Astrocytoma Jorge. A Lazareff H-MRSI and pediatric low grade astrocytomaPediatric brain tumorsThe most common solid cancer of childhood, occurs almost as often as ALL (2.4 vs 2.9/100.000). The most common form of PBT are low grade astrocytomas (30%-35%). Biologie of GliomasLOW GRADE: -Labeling index 1% -S-phase fraction 1% -Growth fraction 2%-6% -Protein synthesis ratio 1 -Ki-index 0%-4.5% HIGH GRADE: -Labeling index 5%-15% -S-phase fraction 5%-20% -Growth fraction 9%-47% -Protein sinthesis ratio 2 -Ki-index 1.7%-32.2% Pediatric low grade AstrocytomaCerebral hemispheres Optic tracts/ hypothalamus Thalamus Intraventricular Brain Stem Cerebellum For many low grade astrocytomas the best treatment is surgery alone. The next pictures clearly show that it is possible to completely remove hemispheric tumors. 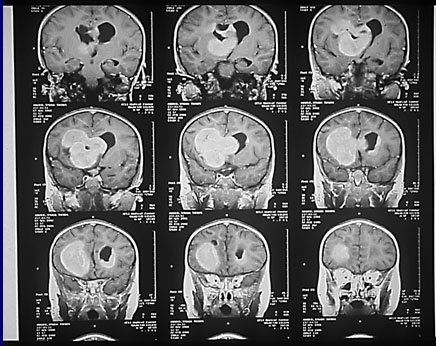 But in some ocassions the tumor can dissapear without any treatment. Those are rare cases, but raise the question about what to do when surgery is not possible, as in the next case. Pilocytic astrocytoma of the optic tract. Surgery will cause severe damage to the child. 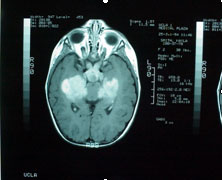 3 months after the previous picture, and without treatment the tumor has almost dissapeared. The child did not have fibromatosis. 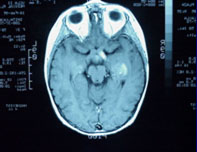 So when we offer treatment we actually might not be offering any valid alternative as in the cartoon bellow. So, how can we know when to be aggressive with a low grade astrocytoma that can not be surgically removed. For that we use spectroscopy.Multivoxel analysis of tumor metabolism. Here we see that the same tumor has different Choline signal intensity in different areas. 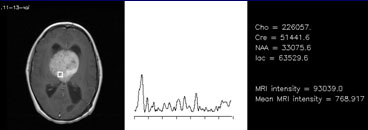 The Choline peak is the first at the left. Note how high is in the above voxel 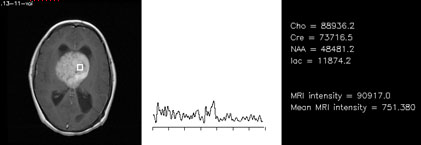 Then we compare the tumor value with the value of the normal brain, and we construct a Normalized Choline value; when it is above 1 it means that there is more choline in the tumor than in the normal brain 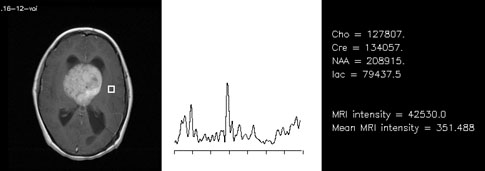 The next pictures shows that those tumors that have a normalized choline above 1 usually progress. 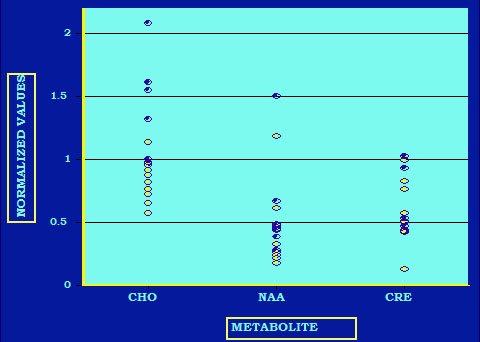 So by calculating the Choline index whe can determine when to be aggressive with chemo and or radiation. Also tumor heterogeneitycan help us in the design of an experimental treatment.If some areas of the tumor have more Choline than others,then lets target those areas with a gamma knife or a linear accelerator. 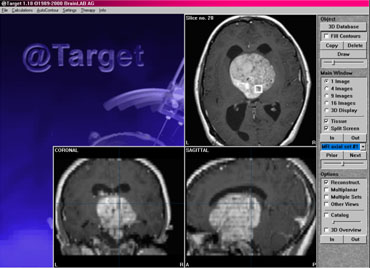 Here you see how we targeted only the high choline areas of a large tumor that otherwise will not be a candidate for gamma knife. The choline value (on the y) shows that it was above 1 before treatment (arrow) and it later dropped to bellow 1 and the tumor stop progressing. 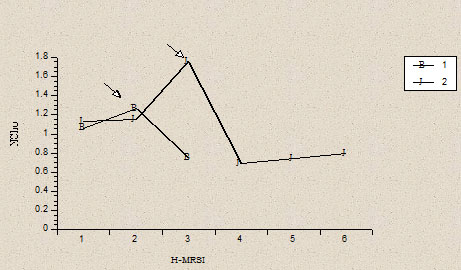 The following two pictures show that a child with a brain stem tumor has a very low choline, we did not treat her at all and one year after-as predicted by the MRS-the tumor is shrinking. 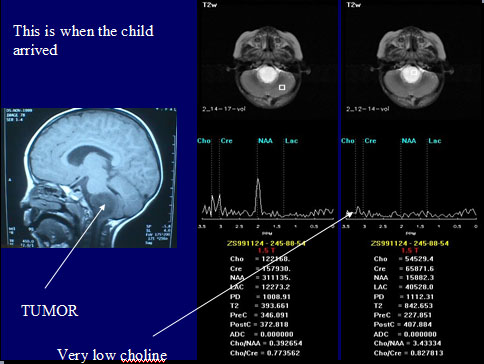 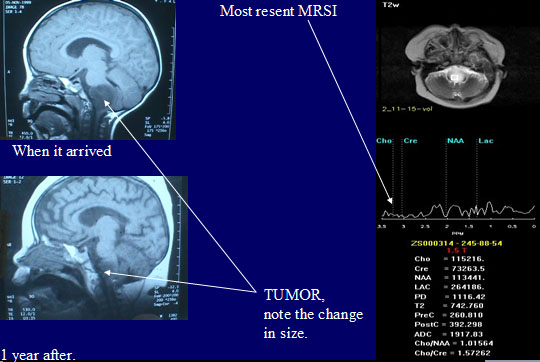 |
||
|
|
© Nicole Delépine - Biographie - Avocat famille Angers - Webangelis - Voyance |